Anatomy of the Fascia System
The sinew channels are full body continuous pathways. For clinical purposes we work with six divisions, not twelve, because the arm and leg aspects of each division are one connected line. What this means practically is that a charge introduced anywhere along the line travels the entire trajectory. Under sympathetic activation these lines contract, flex, or freeze. When the body is in a state of parasympathetic safety they release, and that release is bilateral and runs the full length of the channel every time.
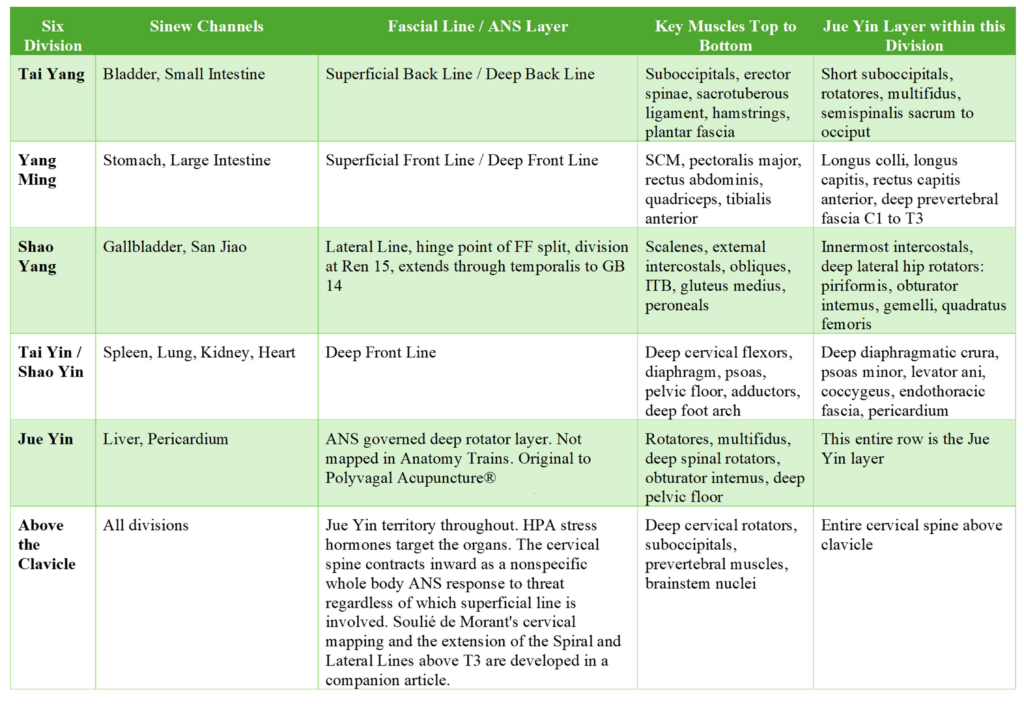
 The Tai Yang sinew channels, Bladder and Small Intestine, correspond to both the Superficial Back Line and the Deep Back Line. The arm and leg aspects are one continuous line and for clinical purposes they are treated as such. This is the posterior longitudinal chain running from plantar fascia through the hamstrings, sacrotuberous ligament, erector spinae, and suboccipitals to the forehead. It governs spinal extension and upright posture. Under sympathetic activation and in retained freeze the posterior chain braces and compresses around the spinal cord, with the deep layer, the rotatores and multifidus, rotating inward to protect the central nervous system while the superficial erectors lock into extension. The Jue Yin layer within Tai Yang is the transversospinalis group from sacrum to occiput, the deepest posterior muscles responding to ANS state rather than to voluntary motor command.
The Tai Yang sinew channels, Bladder and Small Intestine, correspond to both the Superficial Back Line and the Deep Back Line. The arm and leg aspects are one continuous line and for clinical purposes they are treated as such. This is the posterior longitudinal chain running from plantar fascia through the hamstrings, sacrotuberous ligament, erector spinae, and suboccipitals to the forehead. It governs spinal extension and upright posture. Under sympathetic activation and in retained freeze the posterior chain braces and compresses around the spinal cord, with the deep layer, the rotatores and multifidus, rotating inward to protect the central nervous system while the superficial erectors lock into extension. The Jue Yin layer within Tai Yang is the transversospinalis group from sacrum to occiput, the deepest posterior muscles responding to ANS state rather than to voluntary motor command.
The Yang Ming sinew channels, Stomach and Large Intestine, correspond to both the Superficial Front Line and the Deep Front Line. The arm and leg aspects are one continuous line and for clinical purposes they are treated as such. This is the anterior chain from the dorsum of the foot through the quadriceps, rectus abdominis, pectoralis major, and sternocleidomastoid. It governs trunk flexion and neck extension. In freeze it becomes the primary anterior crush pattern, the forward head, elevated chest, jaw bracing, and anterior trunk compression that locks the body into the turtle posture. The Yang Ming line is the fascial expression of the freeze response in the anterior body.
to both the Superficial Front Line and the Deep Front Line. The arm and leg aspects are one continuous line and for clinical purposes they are treated as such. This is the anterior chain from the dorsum of the foot through the quadriceps, rectus abdominis, pectoralis major, and sternocleidomastoid. It governs trunk flexion and neck extension. In freeze it becomes the primary anterior crush pattern, the forward head, elevated chest, jaw bracing, and anterior trunk compression that locks the body into the turtle posture. The Yang Ming line is the fascial expression of the freeze response in the anterior body.
The Shao Yang sinew channels, Gallbladder and San Jiao, correspond to the Lateral Line. This runs along the side of the body through the peroneals, iliotibial band, gluteus medius, obliques, and intercostals. It governs lateral stability and rotation. In a fight or flight model it becomes the hinge point where the split occurs, flight loading below and fight loading above, with the division at Ren 15 where the diaphragm and great vessels cross. The Lateral Line does not terminate at the shoulder. It continues through the scalenes, SCM, and temporalis to GB 14 at the forehead, passing through the throat centers and the lateral cervical chain. The temporalis and jaw are part of the threat detection complex through CN V and the trigeminal system. Until the full length of the Lateral Line releases through the neck and jaw, the brainstem continues to read threat and neither volitional movement nor upright postural organization can come back online. The extension of the Shao Yang line above T3 and its relationship to the cervical spine and brainstem nuclei is developed in a companion article.
The Tai Yin and Shao Yin sinew channels, Spleen, Lung, Kidney, and Heart, correspond to the Deep Front Line. This is the core myofascial chain connecting the deep foot arch through the adductors, pelvic floor, psoas, diaphragm, pericardium, and deep cervical flexors. It is the deepest of the longitudinal lines and the first layer at which autonomic and visceral patterning becomes accessible through manual work. Below the knee the medial yin channels run in such close proximity through the same deep medial compartment that they are not clinically distinct. In a retained freeze response the tendons through the pelvis and medial knee that should be anatomically separate present as one fused structure, a coaxial cable of compressed tissue that bunches like a shower curtain pulled up, cutting off the inguinal arterial supply to the lower limb. Individual channel differentiation becomes relevant again at the feet, and above the knee as the channels diverge into distinct trunk territory.
The Jue Yin layer is different in kind from the lines above it. The muscles that belong here, the rotatores, multifidus, and deep spinal rotators, do not appear in the Anatomy Trains schema. Myers acknowledged this directly: the deep lateral rotators do not fit his line-based model because their fiber direction is orthogonal to the longitudinal lines he was mapping. He noted the fascial connection and set them aside. In this framework they are not set aside. They are the layer that activates in freeze to rotate inward and compress around the spinal cord to protect the brain and the central nervous system. They are not under voluntary control. They do not respond to movement or conscious engagement. They respond to ANS state change only, and they are laid down in the perinatal window under the governance of the primitive reflexes and the cranial nerves. In this framework Jue Yin means the muscle layer governed directly by the ANS, present beneath every division, activated as a unit in freeze regardless of which superficial line is dominant.
kind from the lines above it. The muscles that belong here, the rotatores, multifidus, and deep spinal rotators, do not appear in the Anatomy Trains schema. Myers acknowledged this directly: the deep lateral rotators do not fit his line-based model because their fiber direction is orthogonal to the longitudinal lines he was mapping. He noted the fascial connection and set them aside. In this framework they are not set aside. They are the layer that activates in freeze to rotate inward and compress around the spinal cord to protect the brain and the central nervous system. They are not under voluntary control. They do not respond to movement or conscious engagement. They respond to ANS state change only, and they are laid down in the perinatal window under the governance of the primitive reflexes and the cranial nerves. In this framework Jue Yin means the muscle layer governed directly by the ANS, present beneath every division, activated as a unit in freeze regardless of which superficial line is dominant.
This mapping is original to Polyvagal Acupuncture® and emerged through the author’s own primitive reflex integration work and clinical observation across the trauma population. Myers did not map the deep rotators because his system was built for voluntary movement and biomechanical load transfer. These muscles do not participate in that system. They sit outside it by design.
The point prohibitions in classical texts are not arbitrary cautions. They are clinical observations about what happens when a charge moves through a continuous fascial pathway. An example of why this matters is GB 21, which is listed as a forbidden point during pregnancy. Strong stimulation at GB 21 sends a charge down the full Shao Yang line. That charge travels through the lateral fascial sling, releases the obliques, and causes the pelvic floor to let go. During pregnancy this risks destabilizing the broad ligament, the uterine ligaments, and the pelvic floor support of the uterus itself. It can initiate early labor or compromise the structural support of the fetus. The point prohibition is not arbitrary. It is a description of what happens when you drive a charge down a continuous fascial pathway that runs from the shoulder to the foot.
The Secondary Vessels and the Developmental Record
The QIAO and WEI vessels become active after birth. This is consistent with their clinical territory. The postnatal developmental window is where the vestibular system, the limbic system, the immune system, and the enteric nervous system complete their organization. It is where myelination proceeds, where primitive reflexes are meant to integrate, and where the foundational autonomic patterns are laid down.
The classical literature described the QIAO and WEI vessels as governing mental emotional conditions. This was accurate clinical observation. What the classical physicians were seeing was the somatic record of that developmental period written into the tissue as retained reflexes, autonomic patterning, and fascial organization that has never fully discharged. They had the clinical picture right. They did not have the developmental neuroscience to name what they were seeing.
The Four Myofascial Slings
The slings are where the interaction between the sinew lines becomes visible as a physical loading pattern in the tissue.
The anterior oblique sling connects the external and internal obliques to the contralateral adductors across the pubic symphysis. The posterior oblique sling connects the latissimus dorsi to the contralateral gluteus maximus thro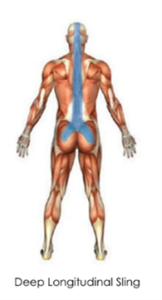 ugh the thoracolumbar fascia. The lateral sling runs through the gluteus medius, tensor fasciae latae, and contralateral adductors. The deep longitudinal sling connects the erector spinae, multifidus, sacrotuberous ligament, and biceps femoris. These slings cross the sinew lines. Under a retained freeze pattern they load simultaneously, and the compression becomes a cube of tissue rather than a line of tension.
ugh the thoracolumbar fascia. The lateral sling runs through the gluteus medius, tensor fasciae latae, and contralateral adductors. The deep longitudinal sling connects the erector spinae, multifidus, sacrotuberous ligament, and biceps femoris. These slings cross the sinew lines. Under a retained freeze pattern they load simultaneously, and the compression becomes a cube of tissue rather than a line of tension.
The JUEYIN Layer
The JUEYIN layer is the deepest fascial architecture in the body. It is laid down in the same perinatal window as the QIAO and WEI vessels, under the governance of the primitive reflexes and the cranial nerves, but it is not the developmental record. It is the substrate beneath it. As weight bearing begins and the frame has to support increasing load, the collagen content rises and the fascia stiffens around the deep rotational musculature that provides stability from the inside out.
In TCM the Liver is described as the general, the arbiter of the body’s defensive pathways. The armed forces the general commands are the sympathetic nervous system. This is not a metaphor. It is a functional correspondence.
This layer is not under voluntary control. Because the sinew channels, the fascia, and the nervous system develop together in the same perinatal window, what is held here is not accessible through conscious intention. Sensory experience and the interpretation of that experience leave a charge in the nervous system. When that charge is never resolved it becomes the basis of autonomic patterning, muscle tone imbalance, and the postural reflexes that organize the body around retained threat. This is what somatic therapists have long recognized as character structure. It is written into the nervous system first and the tissue second. The deep rotators, the structures that organize the spine and support upright posture from the inside out, are governed by this same architecture. They require manual work to reach. For the purposes of this approach we attribute this entire layer to JUEYIN.
Beneath all of this, the autonomic nervous system constantly monitors incoming sensory data against prior experience, below conscious thought, moment by moment. When the input is not threatening the parasympathetic system stays on, the green light for rest, repair, growth, and development. When it is threatening the sympathetic system activates and the body has to deal resolve the threat and return to a parasympathetic baseline. Trauma, whether medical or relational, in the perinatal to five-year window has the potential to remain lodged in the system as an unresolved threat. This is what creates the downstream issues that present clinically later.
What Retained Fight, Flight, and Freeze Actually Does to the Body
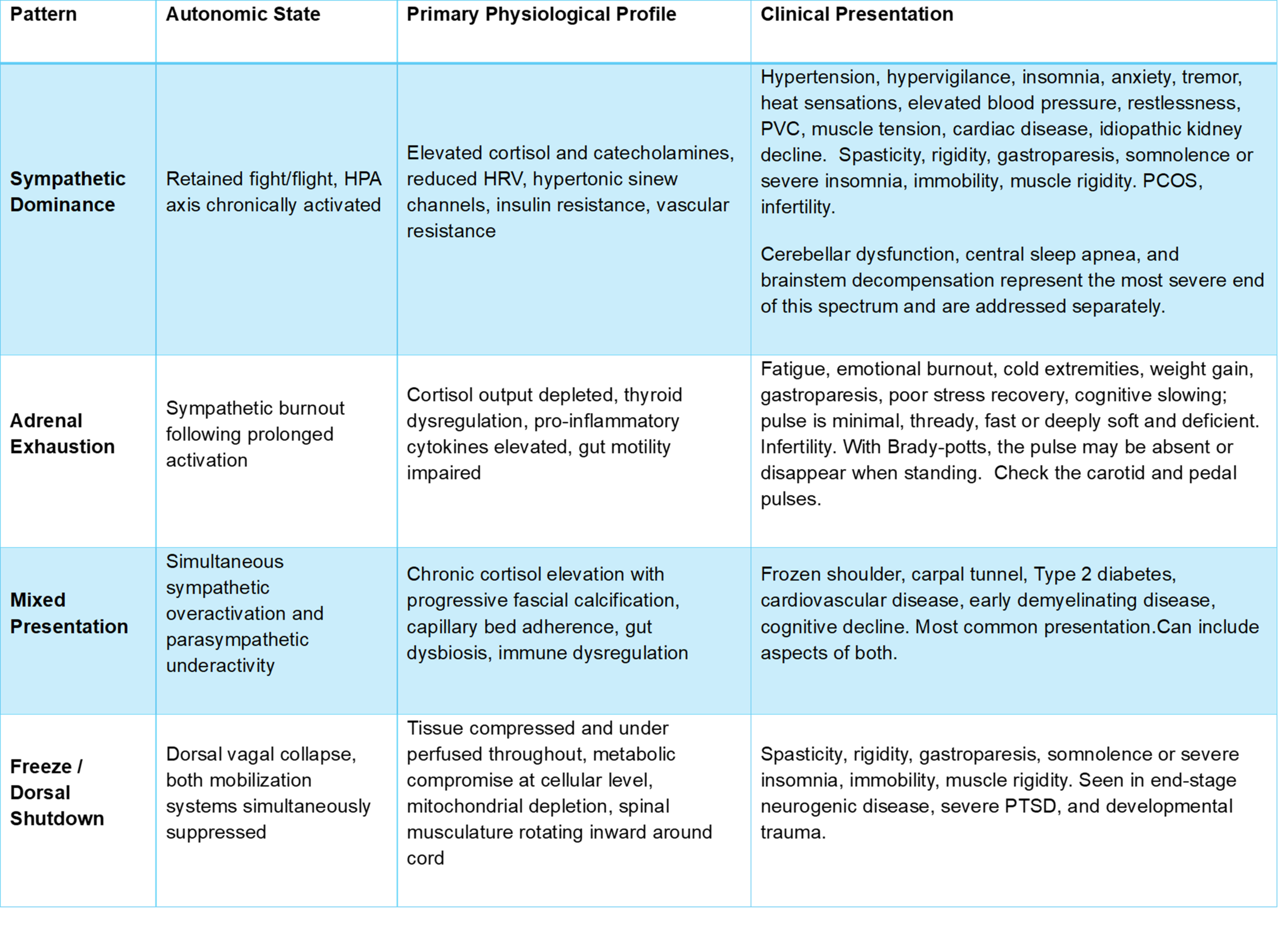
The autonomic nervous system does not store threat abstractly. It stores it as a specific physiological state, and each state leaves a different signature in the tissue. Fight, flight, and freeze are not interchangeable terms for stress. They are distinct mobilization patterns with distinct tissue consequences and conflating them produces clinical errors.
In a flight response, cortisol and adrenaline redirect blood flow and vital fluids to the large skeletal muscles of the lower body, the legs, for running. The lower body becomes the priority. Upper body and organ perfusion are reduced. The pelvic floor braces. The hip flexors load. The lower limb fascial lines go into tension to support propulsive movement that never happens when the response is retained.
fluids to the large skeletal muscles of the lower body, the legs, for running. The lower body becomes the priority. Upper body and organ perfusion are reduced. The pelvic floor braces. The hip flexors load. The lower limb fascial lines go into tension to support propulsive movement that never happens when the response is retained.
In a fight response, the redistribution reverses. Blood and vital fluids are shunted to the upper body, the arms, the jaw, the upper thorax. The upper reflexes dominate: the Moro extension pattern, the tonic labyrinthine reflex in extension, the STNR with elevated shoulders and forward head. The lower body is deprioritized. The upper thorax and cervical region compress.
 Freeze is neither. It is the collapse of both systems simultaneously, the dorsal vagal shutdown that follows when both fight and flight have failed. Cortisol remains chronically elevated but without the directed mobilization of either prior response. Tissue becomes compressed, underperfused, and metabolically compromised throughout. The deep internal rotators curl inward, compressing around the spinal cord in protection. The body’s diaphragms crush inward and upward. If this response never fully discharges, the compression becomes chronic. Tissue calcifies at JUEYIN depth, and the body loses access to the breathing centers of the cervical spine, the proper descent of the vagus nerve, and the proper dissemination of charge through the spinal ganglia.
Freeze is neither. It is the collapse of both systems simultaneously, the dorsal vagal shutdown that follows when both fight and flight have failed. Cortisol remains chronically elevated but without the directed mobilization of either prior response. Tissue becomes compressed, underperfused, and metabolically compromised throughout. The deep internal rotators curl inward, compressing around the spinal cord in protection. The body’s diaphragms crush inward and upward. If this response never fully discharges, the compression becomes chronic. Tissue calcifies at JUEYIN depth, and the body loses access to the breathing centers of the cervical spine, the proper descent of the vagus nerve, and the proper dissemination of charge through the spinal ganglia.
The Clinical Patterns of Retained Dysregulation
There has been no treatment in any modality that consistently restores function to the dysregulated autonomic nervous system. The patterns described below use physiological and symptomatic language only. Sixty years without rigorous funding or research standards in the West have allowed TCM to drift toward abstraction and magical thinking. This is not happening in China or Japan where the medicine is held to a more rigorous clinical standard. The distortion is a Western problem. Using TCM pattern language to describe autonomic dysregulation states opens the door to that distortion and closes the door to communication with every other discipline that needs to be in the room. These patterns belong to the physiology. The language that describes them needs to match. This framework was developed for developmental trauma (DTD), the most treatment-resistant presentation on the autonomic dysregulation spectrum. The hardest case built the method. The application is simpler than the background implies.
Pattern Differentiation and Clinical Presentation
TCM pattern differentiation is worth defining precisely for readers outside the tradition. A TCM pattern is not a Western disease category. It is a cluster of symptoms, signs, and physiological states that co-occur because they share a common underlying mechanism. A typical presentation in this population is the boomer-aged patient who arrives managing acid reflux on a PPI, dumping syndrome following cholecystectomy, Type 2 diabetes on a GLP-1 agonist, hypertension, ED and early idiopathic renal decline, each condition treated separately by a different specialist, each prescription managing one variable in isolation. In this framework those are not five problems. They are one pattern with five expressions, and as the correct pattern is addressed the cluster resolves together because the symptoms were never separate to begin with. In the context of autonomic dysregulation, where a single dysregulated state produces symptoms across every system the ANS governs, pattern differentiation is precisely the right diagnostic tool. Because the substrate is shared across all four patterns, the treatment method is uniform, with specific modifications for the freeze and dorsal shutdown presentations.